
Image Sharpness
In radiography, the aim is to produce an image that is as sharp as possible in order to resolve fine detail within the image. This is particularly important when looking for subtle fractures or changes in bone architecture.
Unfortunately, there are several factors that lead to image
unsharpness. These are unsharpness due to:
• geometry (Ug);
• movement (Um);
• absorption (inherent factors) (Ua);
• photographic/acquisition factors (Up).



Various accessories can be used for immobilization, including non-opaque pads and sandbags to immobilize the extremities.

Binders and Velcro straps may be used for the trunk and head. These accessories should be available in all examination rooms and should be used routinely. It is equally important to make the patient as comfortable as possible and to explain the procedure fully. The radiographer can also invite questions about the procedure, thus increasing the likelihood of achieving full cooperation from the patient. It may be worthwhile rehearsing respiratory manoeuvres prior to an actual exposure being made.
This is due to the shape of the structures in the body. As illustrated, unless the structure has a particular shape, with its edges parallel to the diverging beam, then absorption of the X-ray beam will vary across the object. Considering a spherical object of uniform density, then absorption will be greatest at the centre and
least at the periphery due to the difference in thickness. This gradual fall-off in absorption towards the edges leads to the image having an ill-defined boundary called absorption unsharpness, particularly as most structures in the body have a round edge. Little can be done to reduce this type of unsharpness, apart from increasing image contrast or using digital edge-enhancement techniques.

with increasing distance between the crystal and the film (poor film/ screen contact). Duplitized film with the emulsion on both sides of the film base is commonly used to decrease the exposure given to the patient, but the unsharpness will be greater than if a single-sided emulsion is employed. This is caused by the image
on one side of the emulsion crossing over to the other side. As it does so, the light diverges and produces an image slightly larger than the image on the opposite side. Another possible cause of unsharpness in duplitized films occurs when the final image is
viewed. If the observer is in such a position that the images on each side of the emulsion are not exactly superimposed, this introduces further unsharpness known as parallax.

Photographic unsharpness is reduced by ensuring that all cassettes maintain good film/screen contact and by using fine-grained screens or single-sided emulsions when appropriate. The least photographic unsharpness occurs when intensifying screens are not used, but this is unjustifiable for the majority of radiographic examinations.
Complex formulae have been given to calculate the total unsharpness due to several contributory factors. These show that if any one type of unsharpness is much greater than the others, then only by reducing that type will any significant improvement
be made in image sharpness. For example, when dealing with a restless patient, the greatest source of unsharpness will be the patient movement, and image sharpness will not be improved visibly by reducing other sources of unsharpness.
A summary of the methods used to reduce different types of unsharpness is shown in the table below.
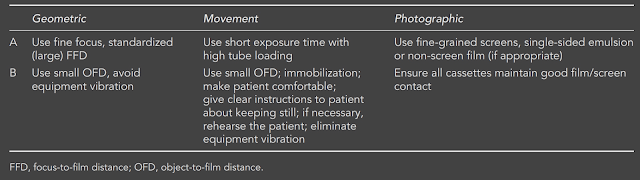
Unfortunately, the factors in group A are interrelated, and attempts to reduce one form of unsharpness will tend to increase another.
For example, if one chooses to use fine-grained screens to reduce photographic unsharpness, then an increase in mAs may be required, which could lead to a longer exposure time, thus increasing the possibility of movement unsharpness. This increase in mAs may in turn require an increase in focal spot size due to the additional thermal stresses on the anode, and there will be an increase in geometric unsharpness as a consequence of this. Choice of factors in group A is part of the radio-grapher’s skill. If movement unsharpness will be a predominant factor,
e.g. with a restless patient, then it must be reduced, perhaps by using a higher tube loading on the broad focus or by the use of the faster intensifying screen to reduce exposure time. In the former situation the geometric unsharpness will increase, and in the latter situation photographic unsharpness will increase. If the patient can be fully immobilized, then the above strategies may not have to be used and an image with a greater degree of sharpness will be obtained.
If we examine the factors in group B, we find that reducing any type of unsharpness with these does not cause another type of unsharpness to increase. For example, by having good film/screen contact, then neither movement nor geometrical unsharpness is increased. There is no increase in geometrical unsharpness or photographic unsharpness if the patient is immobilized.
To obtain the sharpest image possible, we must make a judgement about the factors in group A. We have to decide whether we will use the broad or fine focus, fine-grain or regular/fast screens. But there are no decisions to make about the factors in the group B. We should always strive to position the part under examination as near as possible to the cassette, to immobilize
the patient in as comfortable position as possible, and to give the patient clear instructions and check their understanding of these instructions. All film cassettes should be maintained to ensure good film/screen contact, and other imaging equipment should be maintained regularly.
Unfortunately, there are several factors that lead to image
unsharpness. These are unsharpness due to:
• geometry (Ug);
• movement (Um);
• absorption (inherent factors) (Ua);
• photographic/acquisition factors (Up).
Geometric unsharpness
If X-rays originated from a point source, then a perfectly sharp image would always be obtained. In an X-ray tube, however, the X-rays are produced from the small area of the focal spot on the anode. As can be seen from the diagram below, this leads to the formation of penumbra or ‘partial shadows’ at the edge of the object; it is this that gives rise to geometric unsharpness.
The degree of geometric unsharpness increases with an increased focal spot size and increased object-to-film distance:

Geometric unsharpness can be a small, insignificant quantity if the object is close to the film and a small focal spot is used. For instance, with a postero-anterior projection of the wrist, where the maximum object film distance is about 5 cm, and if a normal FFD of 100 cm is used, then geometric unsharpness is only 0.05 mm using a 1-mm focal spot and only 0.1 mm with a 2-mm focal spot. When thicker parts of the body are being examined, which might require the use of a larger (broad) focal spot, then geometric unsharpness can make a significant contribution to total image unsharpness owing to the greater object-to-film distance.The degree of geometric unsharpness increases with an increased focal spot size and increased object-to-film distance:



Movement unsharpness
This type of unsharpness is due to patient, equipment or film movement during the exposure. Patient movement may be involuntary, e.g. owing to heartbeat or peristalsis, or it may the type of movement that may be controlled by immobilization. It
is important to note that any patient movement is magnified on the image because of the space between the moving object and the film. Sharpness can be increased by using a shorter exposure time (achieved by a lower mAs with higher kVp, higher mA, or greater tube loading), by a small object-to-film distance and particularly by immobilization.
Various accessories can be used for immobilization, including non-opaque pads and sandbags to immobilize the extremities.

Binders and Velcro straps may be used for the trunk and head. These accessories should be available in all examination rooms and should be used routinely. It is equally important to make the patient as comfortable as possible and to explain the procedure fully. The radiographer can also invite questions about the procedure, thus increasing the likelihood of achieving full cooperation from the patient. It may be worthwhile rehearsing respiratory manoeuvres prior to an actual exposure being made.
Absorption unsharpness
least at the periphery due to the difference in thickness. This gradual fall-off in absorption towards the edges leads to the image having an ill-defined boundary called absorption unsharpness, particularly as most structures in the body have a round edge. Little can be done to reduce this type of unsharpness, apart from increasing image contrast or using digital edge-enhancement techniques.

Photographic unsharpness
An X-ray image could be formed by the direct action of X-rays on a photographic emulsion, but more usually the X-ray image is first converted into a light image by intensifying screens. This increases the photographic effect of the X-rays and thus allows exposure to be greatly reduced. The intensifying screens contain crystals that fluoresce when irradiated by X-rays. Photographic unsharpness is the spread of light between the crystals and the photographic emulsion. The spread of light will be greater with
larger crystals (regular or fast screens) and will also be greaterwith increasing distance between the crystal and the film (poor film/ screen contact). Duplitized film with the emulsion on both sides of the film base is commonly used to decrease the exposure given to the patient, but the unsharpness will be greater than if a single-sided emulsion is employed. This is caused by the image
on one side of the emulsion crossing over to the other side. As it does so, the light diverges and produces an image slightly larger than the image on the opposite side. Another possible cause of unsharpness in duplitized films occurs when the final image is
viewed. If the observer is in such a position that the images on each side of the emulsion are not exactly superimposed, this introduces further unsharpness known as parallax.

Photographic unsharpness is reduced by ensuring that all cassettes maintain good film/screen contact and by using fine-grained screens or single-sided emulsions when appropriate. The least photographic unsharpness occurs when intensifying screens are not used, but this is unjustifiable for the majority of radiographic examinations.
Complex formulae have been given to calculate the total unsharpness due to several contributory factors. These show that if any one type of unsharpness is much greater than the others, then only by reducing that type will any significant improvement
be made in image sharpness. For example, when dealing with a restless patient, the greatest source of unsharpness will be the patient movement, and image sharpness will not be improved visibly by reducing other sources of unsharpness.
A summary of the methods used to reduce different types of unsharpness is shown in the table below.

Unfortunately, the factors in group A are interrelated, and attempts to reduce one form of unsharpness will tend to increase another.
For example, if one chooses to use fine-grained screens to reduce photographic unsharpness, then an increase in mAs may be required, which could lead to a longer exposure time, thus increasing the possibility of movement unsharpness. This increase in mAs may in turn require an increase in focal spot size due to the additional thermal stresses on the anode, and there will be an increase in geometric unsharpness as a consequence of this. Choice of factors in group A is part of the radio-grapher’s skill. If movement unsharpness will be a predominant factor,
e.g. with a restless patient, then it must be reduced, perhaps by using a higher tube loading on the broad focus or by the use of the faster intensifying screen to reduce exposure time. In the former situation the geometric unsharpness will increase, and in the latter situation photographic unsharpness will increase. If the patient can be fully immobilized, then the above strategies may not have to be used and an image with a greater degree of sharpness will be obtained.
If we examine the factors in group B, we find that reducing any type of unsharpness with these does not cause another type of unsharpness to increase. For example, by having good film/screen contact, then neither movement nor geometrical unsharpness is increased. There is no increase in geometrical unsharpness or photographic unsharpness if the patient is immobilized.
To obtain the sharpest image possible, we must make a judgement about the factors in group A. We have to decide whether we will use the broad or fine focus, fine-grain or regular/fast screens. But there are no decisions to make about the factors in the group B. We should always strive to position the part under examination as near as possible to the cassette, to immobilize
the patient in as comfortable position as possible, and to give the patient clear instructions and check their understanding of these instructions. All film cassettes should be maintained to ensure good film/screen contact, and other imaging equipment should be maintained regularly.